Culture. How do you define it?
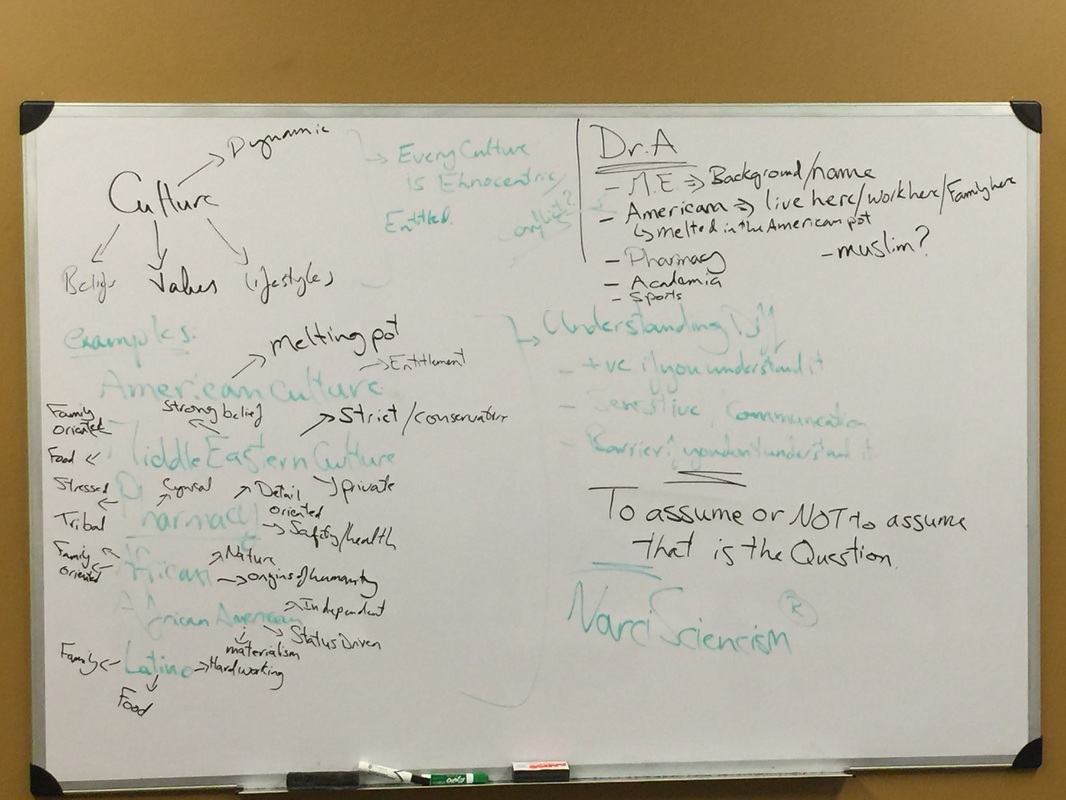
Chap 9 of our book defines culture, and I paraphrase, as a dynamic set of beliefs, values and lifestyle. So based on that definition, I asked the class to give me some examples of cultures
American culture
Middle Eastern culture
African culture
African American culture
Latino culture
Pharmacy culture
Then, after reassuring my students that we are in a safe environment where we are to explore our most often than not subconscious biases, to list what comes to their mind when they think of each of the cultures they mentioned. The answers varied and had the typical mix of sweeping generalization, stereotypes and carefully stated negative assumptions (safe as the environment may be, not everyone is comfortable acknowledging their own biases/prejudices out in the open).
We all have assumptions and generalization about cultures. These assumptions, both positive and negative, come from how we experience culture. Our interactions with a culture, readings about a culture, being part of the culture (we all agreed that as pharmacists we a re a bunch of OCD, anal retentive folks......in our defense though we have to be ) influence how we think of various culture. We also use our own culture as the culture to which we compare every other culture. That, however, is not the main point of today's discussion. The question is What do we do with these perceptions? How do such perceptions influence our interaction with our patients?
I asked the class to identify my culture. What culture would they associate me with?
Middle Eastern- based on background and name
American- since I live and work here and have a family here
Pharmacy (yes, I am anal retentive)
Academia
Sports culture (no I am not a jock)
Muslim? Some hesitation there because they did not know whether to classify my religion as a culture or not
Are Middle Eastern and American contradictory terms? Are they conflicting if you consider one to be conservative and the other as open, melting pot, culture (check yourself here, which culture did you associate with which description?)
What am I? If you consider me a Muslim, and knowing that Muslims are not supposed to drink alcohol, are you going to assume that I do not drink? If you, in your mind, approach me as Middle Eastern, what assumptions would you make about me before you even see me? What if I, as a Muslim healthcare provider, let my faith influence my interaction with my patients?
The point I am driving at is that we, especially as healthcare providers, should check our assumptions and preconceived notions at the door. We need to realize them, acknowledge them and then leave them at the door before we go in to see our patient. we are health care providers. We are to provide care to others equally and not to make assumptions based either on our own cultural beliefs or our assumptions of their cultural beliefs. This might sound like a bunch of philosophical political correctness that has no place in real life but consider the statistics about African Americans, Latino and Whites involvement in decision making with regards to their health. (we, as healthcare providers, suffer from bad case of NarciScienceism to a great extent and tend to "tell" patients how they should care for themselves rather than engage them in their own self-care. That "telling" is more pronounced with minority groups)
Then a great question came. But wouldn't making an assumption help me be more culturally sensitive to the needs of my patient? Understanding how different they are from me would make me a better practitioner. So should I not make any assumptions?
Yes, understanding your patient's cultural needs would definitely make you a better provider. Making an assumption about them and subconsciously passing judgement due to that assumption however will not. The best way is to, again, acknowledge your potential biases and to check your preconceived notions at the door. Treat each patient individually, approach them with cultural humility and understand their own specific needs. I'll use me as an example again. Pre-marital sex in Islam is a sin. If I, as a Muslim healthcare provider, approach my patient interactions in that mindset, that everyone who has pre marital sex is a sinner, then how would my interaction be with the patient? What if that patient was a teenage Muslim girl with an STD?
Acknowledging our subconscious biases and preconceived notions about others, especially in the context of caring for the vulnerable and underserved, is of paramount importance. We must know what additional barriers such biases add to a population that is already having to overcome many barriers.
Ask yourself, how do you view a person? What is your role as a health care provider?
Chap 9 of our book defines culture, and I paraphrase, as a dynamic set of beliefs, values and lifestyle. So based on that definition, I asked the class to give me some examples of cultures
American culture
Middle Eastern culture
African culture
African American culture
Latino culture
Pharmacy culture
Then, after reassuring my students that we are in a safe environment where we are to explore our most often than not subconscious biases, to list what comes to their mind when they think of each of the cultures they mentioned. The answers varied and had the typical mix of sweeping generalization, stereotypes and carefully stated negative assumptions (safe as the environment may be, not everyone is comfortable acknowledging their own biases/prejudices out in the open).
We all have assumptions and generalization about cultures. These assumptions, both positive and negative, come from how we experience culture. Our interactions with a culture, readings about a culture, being part of the culture (we all agreed that as pharmacists we a re a bunch of OCD, anal retentive folks......in our defense though we have to be ) influence how we think of various culture. We also use our own culture as the culture to which we compare every other culture. That, however, is not the main point of today's discussion. The question is What do we do with these perceptions? How do such perceptions influence our interaction with our patients?
I asked the class to identify my culture. What culture would they associate me with?
Middle Eastern- based on background and name
American- since I live and work here and have a family here
Pharmacy (yes, I am anal retentive)
Academia
Sports culture (no I am not a jock)
Muslim? Some hesitation there because they did not know whether to classify my religion as a culture or not
Are Middle Eastern and American contradictory terms? Are they conflicting if you consider one to be conservative and the other as open, melting pot, culture (check yourself here, which culture did you associate with which description?)
What am I? If you consider me a Muslim, and knowing that Muslims are not supposed to drink alcohol, are you going to assume that I do not drink? If you, in your mind, approach me as Middle Eastern, what assumptions would you make about me before you even see me? What if I, as a Muslim healthcare provider, let my faith influence my interaction with my patients?
The point I am driving at is that we, especially as healthcare providers, should check our assumptions and preconceived notions at the door. We need to realize them, acknowledge them and then leave them at the door before we go in to see our patient. we are health care providers. We are to provide care to others equally and not to make assumptions based either on our own cultural beliefs or our assumptions of their cultural beliefs. This might sound like a bunch of philosophical political correctness that has no place in real life but consider the statistics about African Americans, Latino and Whites involvement in decision making with regards to their health. (we, as healthcare providers, suffer from bad case of NarciScienceism to a great extent and tend to "tell" patients how they should care for themselves rather than engage them in their own self-care. That "telling" is more pronounced with minority groups)
Then a great question came. But wouldn't making an assumption help me be more culturally sensitive to the needs of my patient? Understanding how different they are from me would make me a better practitioner. So should I not make any assumptions?
Yes, understanding your patient's cultural needs would definitely make you a better provider. Making an assumption about them and subconsciously passing judgement due to that assumption however will not. The best way is to, again, acknowledge your potential biases and to check your preconceived notions at the door. Treat each patient individually, approach them with cultural humility and understand their own specific needs. I'll use me as an example again. Pre-marital sex in Islam is a sin. If I, as a Muslim healthcare provider, approach my patient interactions in that mindset, that everyone who has pre marital sex is a sinner, then how would my interaction be with the patient? What if that patient was a teenage Muslim girl with an STD?
Acknowledging our subconscious biases and preconceived notions about others, especially in the context of caring for the vulnerable and underserved, is of paramount importance. We must know what additional barriers such biases add to a population that is already having to overcome many barriers.
Ask yourself, how do you view a person? What is your role as a health care provider?
